Entrustable Professional Activities
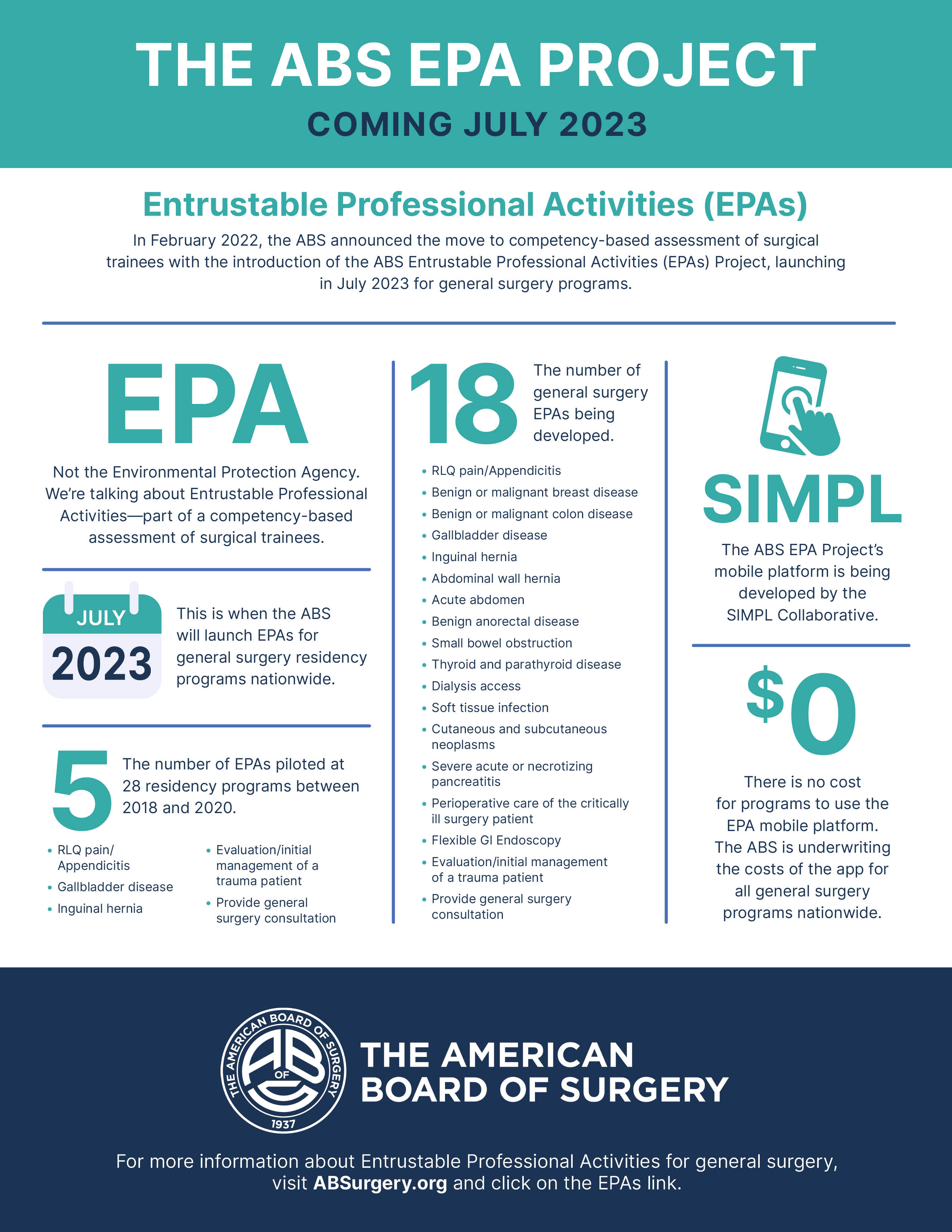
- In February 2022, ABS announced the move to competency-based assessment of surgical trainees with the introduction of the ABS Entrustable Professional Activities (EPA) Project, launching in July 2023 for general surgery residency programs.
- The 18 General Surgery EPAs are now available for viewing. View them here, or view a combined document that includes all 18 EPAs aligned with the applicable ACGME Milestones here.
What is an EPA?
- Entrustable Professional Activities (EPAs) were developed to provide the opportunity for frequent, time-efficient, feedback-oriented and workplace-based assessment in the course of daily clinical workflow. EPAs are an important clinical assessment component of competency-based resident education (CBRE). They offer the opportunity to operationalize competency evaluation and related entrustment decisions in the course of regular patient care, and address some of the challenges educators and trainees have faced in bridging core competency theory into clinical practice and performance assessment.
- It is important to note that EPAs are NOT competencies, but rather a complement to competencies, and serve as a way to translate the broad concept of competency into everyday practice.
- EPAs are units of work a physician performs that can be directly observed - things people do, such as evaluating and managing a patient experiencing a specific medical concern.
- Competencies are broad and foundational domains of ability, such as medical knowledge or interpersonal skills.
- Milestones are capabilities that describe progress at advancing levels of competence along the sequence from novice to expertise.
- A suite of EPAs for a specialty can define the core clinical activities that a resident should exhibit to be deemed competent and worthy of autonomy and entrustment in patient care. Because EPAs are anchored in clinical practice, they allow a way to capture the in-the-moment decisions that attending physicians are already making about how much supervision or autonomy they will give a trainee in a real-world setting and can inform the trainee's progress towards entrustment for a patient's care.
The Transition to a Competency-Based Assessment Model
Information about the ABS EPA Project
- For many years, surgery has relied on surrogate measures of competence such as case logs, attestations of program directors, and test performance to infer readiness for independent practice. The resulting educational systems have been time-based rather than based on objective demonstration of necessary competence. By many measures, including graduate self-assessment, board exam performance, post-residency mentor assessment, and patient outcome assessment as a function of residency program of origin, the results have been highly variable and questionably worthy of the public trust accorded the profession.
- Competency and outcomes-focused education has been increasingly advocated for since the mid-20th century, with gathering momentum in medical education over the last quarter century. Features of CBRE alongside EPAs as a workplace-based assessment strategy include curricular reform and expanded use of simulation as an adult-learning appropriate and safe skill development paradigm. Assessment structures that allow direct observation based on frequent evaluation of performance to drive feedback and learning have been recognized, espoused, and piloted in other countries, including at a national level in Canada. Initiatives in U.S.-based GME such as standardized cognitive and skills curricula (SCORE, FLS, FES, ATLS, ACS/APDS Resident Skills Curriculum, ACS/APDS/ASE Residency Prep Curriculum) and competency-oriented accreditation reform (RRC-S requirements for simulation, core competency and milestone assessment, and duty hour regulation) have been driven by this trend.
- In this overall framework of education reform and its goal of producing a more standardized and attestably competent product, EPAs provide the opportunity to create a new habit or pattern of assessment that is:
- Achievable in any context as it is based in already existing clinical patient care;
- Scalable in that it relies on frequent micro-assessment at the time of work already being accomplished, will replace less meaningful and time-consuming practices such as end of rotation evaluations, and will allow automatic population of key documentation elements of resident progression such as milestone maps that inform CCC promotion decisions;
- Relevant through its direct link to the performance of the duties of a surgeon in patient care;
- Adaptable in that it creates a new habit of ongoing feedback and dialog in the clinical performance arena that can teach trainees skills of implementation and improvisation required in the uncertainties of clinical practice; and
- Hippocratic in its commitment to an ongoing and real time-based formation of the next generation of surgeons as a daily menu of training environment behavior.
- Given this vision and in necessary partnership with the whole house of surgery, the ABS will launch EPAs for general surgery in July 2023. EPAs are also in the early stages of development for the other ABS specialties, including vascular surgery, pediatric surgery, complex general surgical oncology, and surgical critical care, with plans to introduce this trainee assessment model to those specialty programs in the coming years as well.
Lessons Learned from the EPA Pilot
- The ABS began exploring EPAs as a potential foundation for competency-based surgical training and initial board certification in 2016, following several years of discussion around various strategies to improve traditional time-based residency training models. The ABS then developed five index EPAs and piloted them at 28 diverse surgical residency programs from 2018-2020. Lessons learned from this pilot are now being collated and formed into best practice strategies that will be deployed in developing and supporting programs of all types and resource streams during implementation of the EPA assessment model.
- With the onset of the COVID-19 pandemic in early 2020, it became more apparent than ever that a move to competency-based assessment is necessary to appropriately determine trainee readiness to enter the ABS certification process and independent patient care. The ABS is currently developing a full suite of EPAs, encompassing the core patient care activities of the specialty, to form the foundation for competency-based assessment of general surgery trainees. All other ABS specialty boards will follow in the coming years.
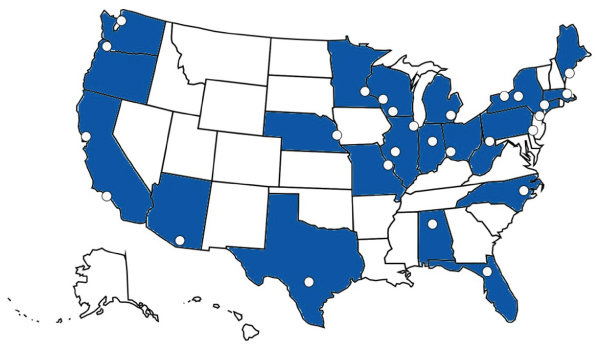
ABS EPA Pilot Program Map
ABS as a Facilitator
- As the organization that sets the standards to achieve certification in several surgical specialties and subspecialties, ABS felt it was appropriate to develop and implement this method of resident and trainee assessment in partnership with other key surgical education organizations as listed below, without whose engagement a reform of this scale would not be possible.
- There are currently two councils and five working groups responsible for the development and implementation of the ABS EPA initiative: the EPA Advisory Council; the EPA Scope Council; the EPA Revision Working Group; the EPA Best Practices Working Group; the EPA Technology Task Force; the EPA Writing Group; and the EPA Development Task Force. All five working groups include resident members who provide valuable insight and recommendations from the trainees' perspective. These groups are currently active for the general surgery project as the first ABS specialty to proceed with implementation of EPAs, with parallel groups for the other ABS specialties already formed or forming for their own specialty-specific processes.
- For a list of volunteers who have been involved in the ABS EPA Project, including pilot programs and working group members, please see here.
EPA Advisory Council
- The EPA Advisory Council oversees the entire EPA project for all ABS specialties and provides much-needed expertise about surgical education and EPAs. This group is comprised of members and representatives from many of our partnering organizations, including a number of program directors from varying program types who were part of the 2018-2020 ABS EPA Pilot.
EPA Scope Council
- The EPA Scope Council used a variety of inputs including existing definitions of the specialty as well as trainee and practicing surgeon case logs to define the final set of 18 general surgery EPAs. Vascular surgery has similarly defined its scope of EPAs, and the other ABS specialty boards will be following with the scoping process as a starting point for EPA development. The goal of the scoping process is to define the foundation of the specialty that can be expected of all trainees in all programs, as framed by current training requirements, practice data, and demographic need, including those domains that are common enough to be meaningfully and reliably assessed in all training environments.
- Once the scoping process is completed, the Scope Council functions as a reactor panel for the full suite of EPAs that are being written by the specialty-specific EPA Writing Group.
EPA Revision Working Group
- The EPA Revision Working Group led the revision of the initial five EPAs evaluated during the 2018-2020 pilot to make them Milestones 2.0 compliant. This group was also responsible for the development of the final entrustment scale, which will be used across all specialty EPA programs. Revision groups will function similarly for other specialty boards as their own EPAs are written and tested in that discipline's training programs.
EPA Best Practices Working Group
- The EPA Best Practices Working Group is responsible for gathering and assessing input from pilot sites as a foundation for "best practice" strategies that will be used in EPA implementation. This group will collaborate with the EPA Development Task Force and the and the Education and Training Committee of the ABS Council to inform the initial EPA training tools for program directors, administrators, faculty, and trainees.
- The work of this group will be amended by iterative learning that occurs through other specialty boards' own implementation processes, though the foundational work done by the original General Surgery Best Practices Working Group is expected to be applicable to programs of all ABS specialty boards.
EPA Technology Task Force
- The EPA Technology Task Force established a list of the essential features of the electronic tools required to implement EPAs in surgical residencies and was responsible for sourcing or developing the application that would be used to track EPAs in all U.S.-based general surgery residency programs.
- Following a thorough review process, the ABS announced in September 2022 that it had selected the SIMPL Collaborative to provide the mobile platform for the ABS EPA Project. The ABS will provide this tool free of charge to all training programs for their use, with priorities around ease and efficiency of use, secure data management, and meaningful dashboard and other outputs to assist learners, programs, and accrediting agencies in their critical work.
- The same tool will be provided for the assessment of EPAs for the other ABS surgical specialties when they are introduced in the coming years.
EPA Writing Group
- The EPA Writing Groups are responsible for the actual creation of all of the EPAs for each specialty area. Each completed EPA includes a description, essential functions, scope and expected behaviors. These groups work in dyads, each writing up to two EPAs. Membership of these groups is broad, and includes members of the various ABS specialty boards, APDS representatives, and residents. There are designated EPA Writing Groups for each ABS specialty area.
EPA Development Task Force
- The EPA Development Task Force is comprised of educators, program directors, residency administrators, and residents, and is developing the actual materials and strategies which will equip programs, faculty, and residents in implementation of the EPAs at the full spectrum of program types. The materials under development will be provided for programs based on insights gained from the EPA Best Practices Working Group, and will be adapted for and used across all ABS specialty areas.
Building on Partnership
ABS is working very closely with several key surgical education partners and stakeholders across the nation to refine the lessons learned from the EPA pilot experience into a full suite of EPAs representative of the core elements of general surgical practice.
Partner organizations engaged in this initiative include:
- Accreditation Council for Graduate Medical Education (ACGME) and the Residency Review Committee (RRC) for various surgical specialties
- Association of Program Directors in Surgery (APDS)
- Association of Program Directors in Vascular Surgery (APDVS)
- Association of Residency Administrators in Surgery (ARAS)
- American College of Surgeons (ACS)
- American Board of Medical Specialties (ABMS) and its member boards
- Association for Surgical Education (ASE)
- American Surgical Association (ASA)
- Fellowship Council (FC)
- Royal College of Physicians and Surgeons of Canada (RCPSC)
- Society of Surgical Chairs
Through surveys, focus groups, and one-on-one discussions, ABS is also engaging current surgical trainees and fellows, as well as the medical student community, to allow these young physicians to share their experiences and have their voices heard during the development of these programs.
Additional Information
This page will be updated with additional information as it becomes available.
For a collection of publications related to the ABS EPA project, please see here.
For a list of volunteers who have been involved in the ABS EPA Project, including pilot programs and working group members, please see here.
If you have any questions about the ABS EPA Project, or have interest in getting involved, please contact our EPA project manager.
